
The groundbreaking, non-invasive metric to evaluate your lung health.
Oxygen Deficit is the most informative and direct way of measuring pulmonary gas exchange efficiency. Calculated as the difference between alveolar oxygen levels in the lungs and the arterial oxygen levels in the blood, Oxygen Deficit is a precise metric of how efficiently oxygen is transported across the blood-gas barrier. 
Assessing the efficiency of gas exchange in patients is an important aspect of clinical management and is done by measuring the difference between the partial pressure of oxygen in the lung and arterial blood. The value of measuring the A-a gradient is well-established, has proven clinical utility, and has been called the most informative index of the efficiency of pulmonary gas exchange.
Oxygen Deficit can be considered a surrogate for the alveolar-arterial gradient, and it paves the way for new advancements in pulmonary medicine. Utilizing a complex algorithm, we combine the directly measured alveolar gas levels and adjust for the Bohr effect in real-time to calculate the blood oxygen level.
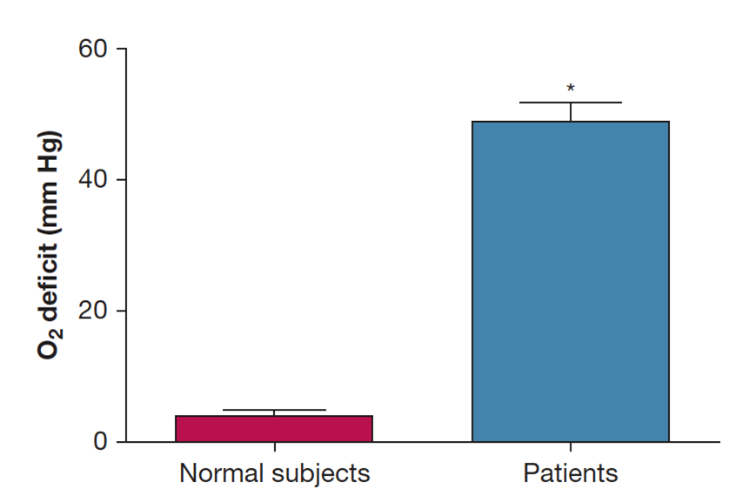
The normal range for Oxygen Deficit is 0-15 mmHg and increases with severity of disease.

The most common explanation for an increased Oxygen Deficit are ventilation-perfusion mismatches, diffusion limitations, and shunting. The normal range for Oxygen Deficit is 0-15 mmHg, depending on age. However, in patients with gas exchange abnormalities, including COPD, heart failure, pneumonia, or influenza-like diseases requiring hospitalization, Oxygen Deficit is significantly increased, with higher values indicating increasing severity of disease.
Oxygen Deficit has very high sensitivity to the presence of lung disease, and has been instrumental in identifying a range of cardiorespiratory complications such as pneumonia, pulmonary fibrosis, pulmonary embolism, and heart failure. Due to its sensitivity, it serves as a great patient safety measure: both in identifying impending respiratory collapse sooner and aiding in differential diagnosis. Using the MediPines AGM100, healthcare providers can accurately identify hypoxemia and quickly narrow its cause, leading to better patient outcomes and higher healthcare system efficiency.
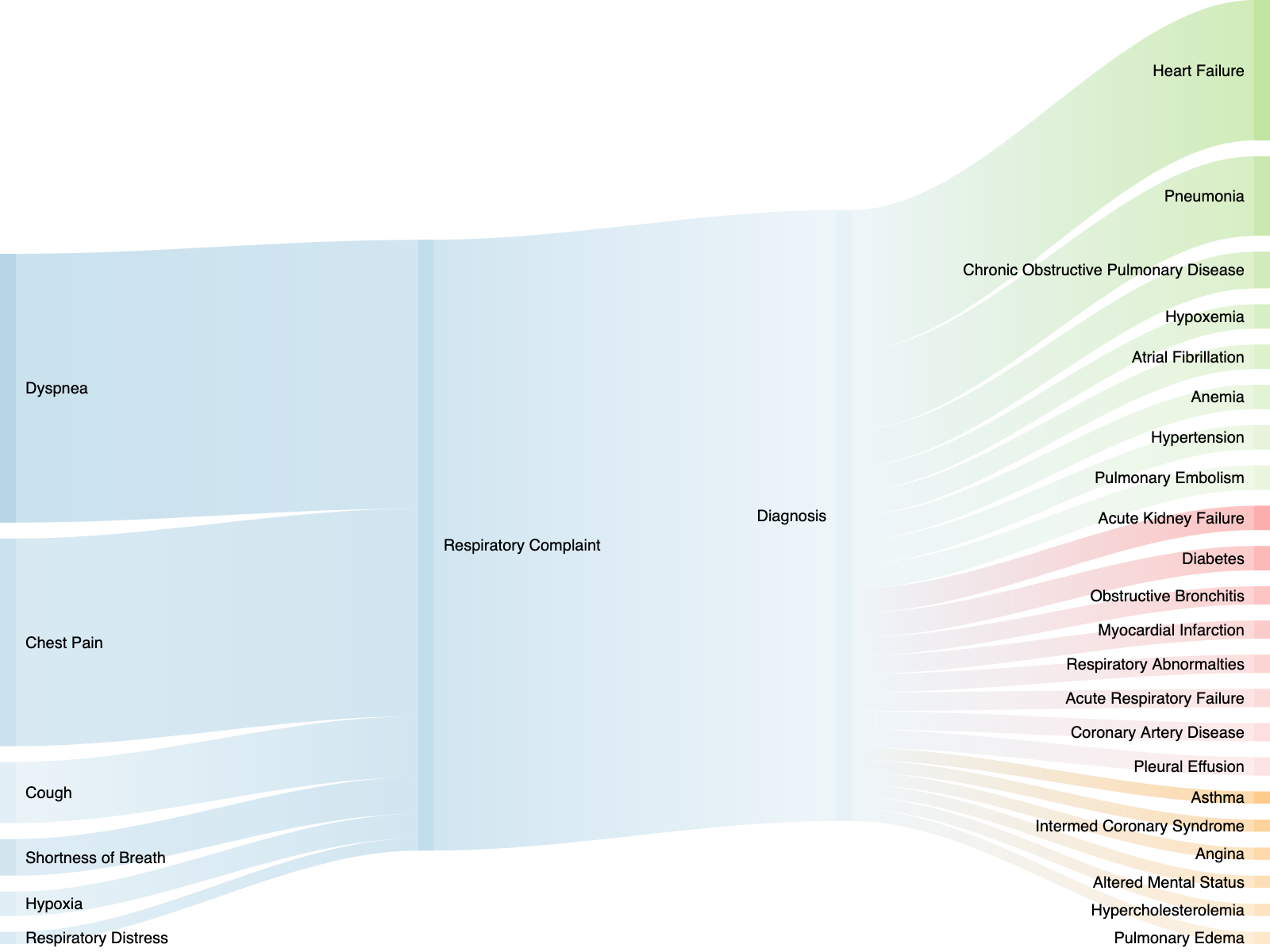
Patients in respiratory distress require immediate medical attention. The ability to quickly identify hypoxemia and its cause is crucial for positive patient outcomes. However, there is a gap in the current cardiorespiratory assessment toolkit that leaves clinicians unable to quickly identify the cause and severity of hypoxemia.
.png?width=300&height=89&name=MP%20Logo_All-in-One_070820%20(1).png)